The Uncertain Optimal Time for Antibiotics in Sepsis
SUMMARY
- Most sepsis treatment protocols call for antibiotic administration as soon as possible.
- This practice may benefit patients with septic shock, it may be detrimental for those without shock.
- Forcing clinicians to sacrifice diagnostic accuracy for speed, may result in the overuse of antibiotics.
BACKGROUND
Advantages of Rapid Antibiotic Administration:
- “Each hour delay in initiating antibiotics costs lives”
- Delay in the initiation of appropriate antibiotic therapy has been recognized as a risk factor for mortality.
- When sepsis is suspected, treat everyone: “just in case”
Disadvantages of Rapid Antibiotic Administration:
- Non-infectious cases of suspected sepsis in the emergency department account for 13-18% of cases
- Antibiotics of no benefit in non-bacterial causes of infection
- Overuse of antibiotics may result in:
o Increased antibiotic resistance
o Organ injury
o Clostridium difficile infections
The first study to report that each hour delay in initiating effective antibiotic therapy was by Kumar et al in 2006. Each hour delay was associated with a 7.6% decrease in survival. Since then numerous other reports and reviews have also found a significant increase in mortality for each hour of antibiotic administration delay. These studies suffer from:
- Significant heterogeneity between sepsis and septic shock patients.
- The major difference of early antibiotic administration on mortality is between sepsis and septic shock patients.
- Retrospective in nature of databases designed for non-clinical purposes (administrative, etc)
- Missing information, such as:
o Confirmation of infection
o Adequacy of antibiotic selection based on sensitivity patterns
o Antibiotic dosing
o Source control
REVIEW
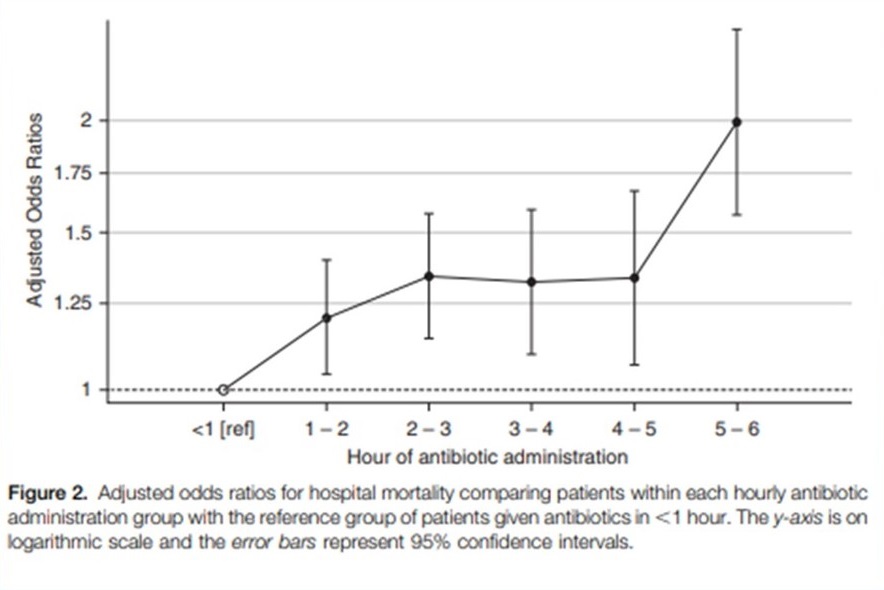
Recently Lui et (2017) retrospectively studied antibiotic administration in 35,000 sepsis patients. Compared to antibiotics given in the first hour, the adjusted odds ratio for hospital mortality between hours 2 to 5 was similar without worsening.
Two prospective studies with emergency department and pre-hospital antibiotic administration have failed to show a mortality benefit from early administration.
- de Groot et al (2015) 1,168 emergency department patients
o Patients segmented into severity score based on PIRO (Predisposition Infection Response and Organ Dysfunction scoring system). Lower value indicates less severity.
o Compared statistical significance of number of surviving days outside of hospital after day 28 of ED presentation
o Antibiotics administered within 1 hour were compared to administration between 1 – 3 hours and greater than 3 hours
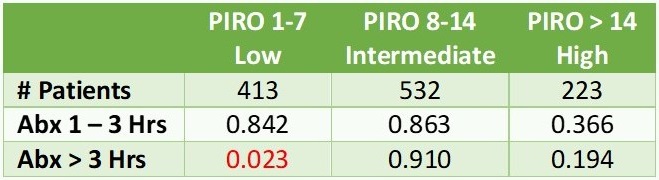
o No association between time to antibiotics and surviving days outside hospital.
o Only the lowest PIRO group given antibiotics greater than 3 hours had a significant increase in survival days.
- Alan et al (2018) 2,672 patients randomized controlled open labeled trial from the Netherlands
o Compared early administration of antibiotics in the ambulance with usual care.
o Evaluated all cause mortality at 28 days

CONCLUSIONS
-
Every suspected sepsis patient should be seen promptly and antibiotics should NOT be unnecessarily delayed.
-
It is reasonable to provide rapid empiric antibiotics to sepsis patients with evidence of shock.
-
Identify patients with suspected sepsis without shock who will not be hurt by additional data to confirm the diagnosis. These patients may not need antibiotics in as quick a time period.
-
Patients not in shock may not need a quick time period for antibiotics.
-
Need a better distinction between bacterial and non-bacterial sources.
To receive articles like these in your Inbox, you can subscribe to Sepsis Program Optimization Insights.
Erkan Hassan is the Co-Founder & Chief Clinical Officer of Sepsis Program Optimization where he designs & oversees the implementation of solutions to optimize sepsis programs.
To discuss your organization’s Barriers of Effective Sepsis Care, contact Erkan by phone (844) 4SEPSIS (844-473-7747), email (erkan@spo.icu), or video chat.



