Mortality with Early vs Late Renal Therapy in
Sepsis Associated Acute Kidney Injury
Summary
- Sepsis is the leading cause of acute kidney injury (AKI) in critically ill patients.
- Timing of renal replacement therapy (RRT) has produced inconsistent results due to poor study designs and inconsistent definitions.
- Early identification and intervention may improve mortality from sepsis-associated AKI.
Background
Sepsis is the leading cause of AKI in critically ill patients, contributing to increased risk of death, prolonged hospitalizations and increased need for renal replacement therapy.
Both sepsis and AKI share the following characteristics:
- Their definitions have evolved over the past 20 years
- They are both caused by numerous etiologies with complex pathophysiologic processes
- They are both associated with a high degree of morbidity and mortality
- Early recognition and intervention are needed to improve outcomes
Review
Optimal timing and outcomes of RRT in sepsis-associated AKI have produced inconsistent and conflicting results. This is due to several limitations within the patient population, study design, and data generated. These limitations include:
- Sepsis associated AKI patients are a clinically heterogeneous group with mixed causes of AKI
- There are no established definitions of what constitutes “early” or “late” RRT
- Published studies suffer from:
o Small sample sizes
o Retrospective nature
o Varying eligibility criteria
o Differing definitions of AKI and early/late RRT timeframes
o Various follow-up periods
The benefits of early RRT include potential earlier recovery of renal function with chemistry and fluid equilibrium, decreased hospital length of stay, and improved survival.
The benefits of late RRT allow for the patient to clinically stabilize and potentially recover renal function without RRT and its potential complications.
Studies demonstrate improved 28-day mortality with early vs late RRT (Table 1) or no benefit from early vs late RRT (Table 2).
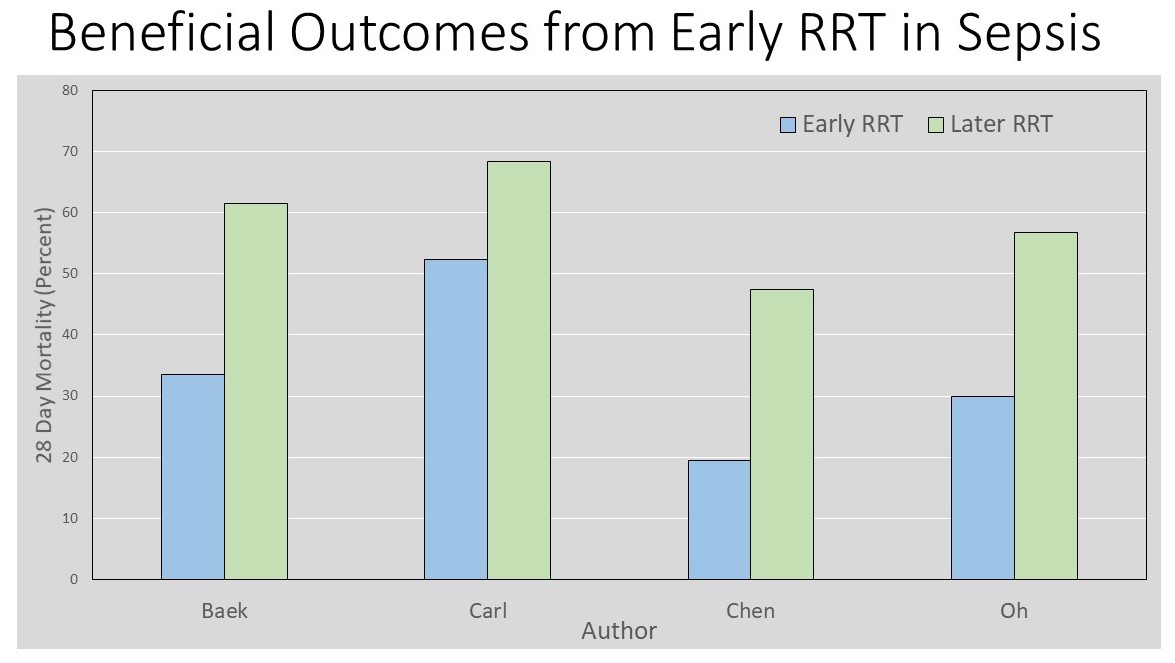
Table 1 Beneficial Outcomes from Early RRT in Sepsis
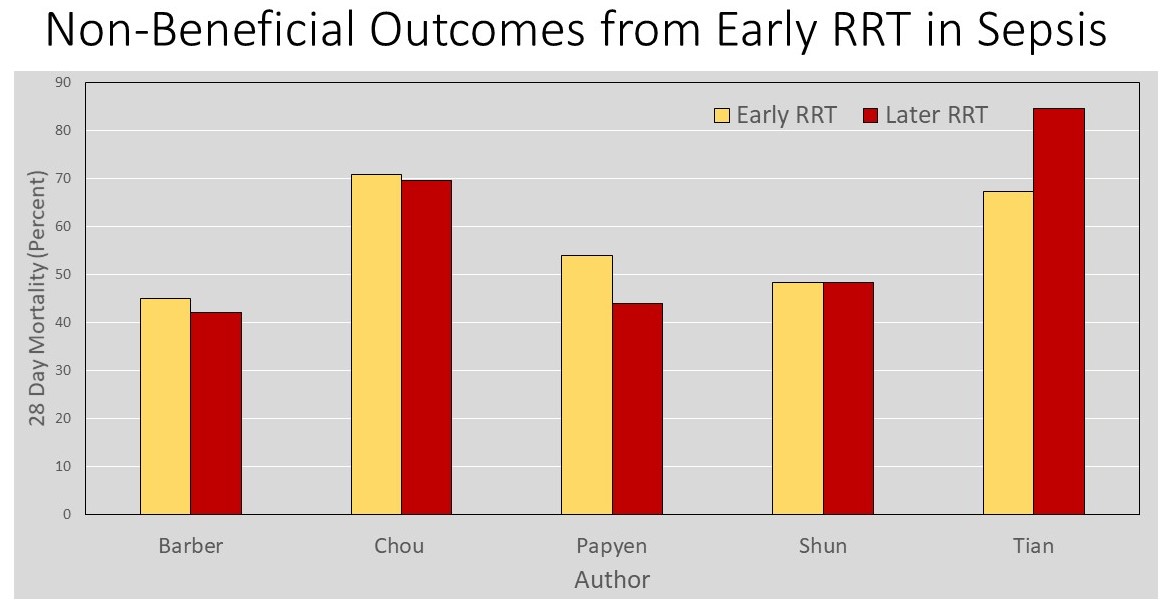
Table 2 Non-Beneficial Outcomes from Early RRT in Sepsis
CONCLUSIONS
- Optimal timing of RRT in sepsis-associated AKI is not clear – large multi-centered prospective studies are needed.
- Timing to start RRT should be individualized based on a patient’s clinical status and laboratory progression.
- Early RRT may potentially improve outcomes.
To receive articles like these in your Inbox, you can subscribe to Sepsis Program Optimization Insights.
Erkan Hassan is the Co-Founder & Chief Clinical Officer of Sepsis Program Optimization where he designs & oversees the implementation of solutions to optimize sepsis programs.
To discuss your organization’s Barriers of Effective Sepsis Care, contact Erkan by phone (844) 4SEPSIS (844-473-7747), email (erkan@spo.icu), or video chat.



